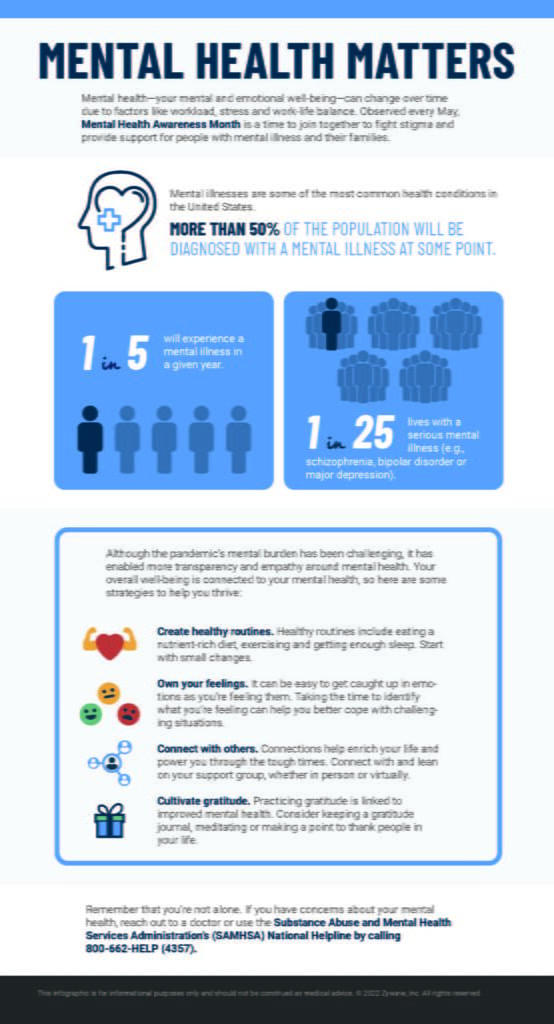
Mental health—your mental and emotional well-being—can change over time due to factors like workload, stress and work-life balance. Observed every May, Mental Health Awareness Month is a time to join together to fight stigma and provide support for people with mental illness and their families.
Cyberattacks are a growing concern for employers across the globe but especially for those in the United States. According to the Identity Theft Resource Center, the number of reported U.S. data breaches rose 68% between 2020 and 2021, increasing to a record-setting 1,862 incidents. Of these breaches, 83% involved sensitive information, such as Social Security numbers.
These breaches targeted various organizations and industries, including those in manufacturing, utility services and finance. Essentially, any business that retains potentially valuable information could be a target; cybercriminals are frequently looking for the personal information of everyday citizens to sell or use to gain access to other systems.
Oftentimes, cybercriminals breach organizations via their own employees; all it takes is one employee clicking into a phishing email (i.e., a fraudulent message intended to trick recipients into compromising important data).
This is where HR comes in. HR teams are often tasked with communicating policy updates and workplace expectations. When it comes to cybersecurity, HR is naturally suited to partner with IT and provide basic educational resources. This article offers tips to help HR teams protect employees and their organizations from cyberattacks.